Biosimilars Generics And The 2026 Medicare Drug Cost Decision
For many Medicare beneficiaries, the word cheaper sounds reassuring. A doctor mentions a biosimilar, a pharmacist suggests a generic, or a Part D plan places one version of a medication on a preferred tier. The natural assumption is that the less expensive drug must be the smarter choice. In 2026, that assumption deserves a closer look.
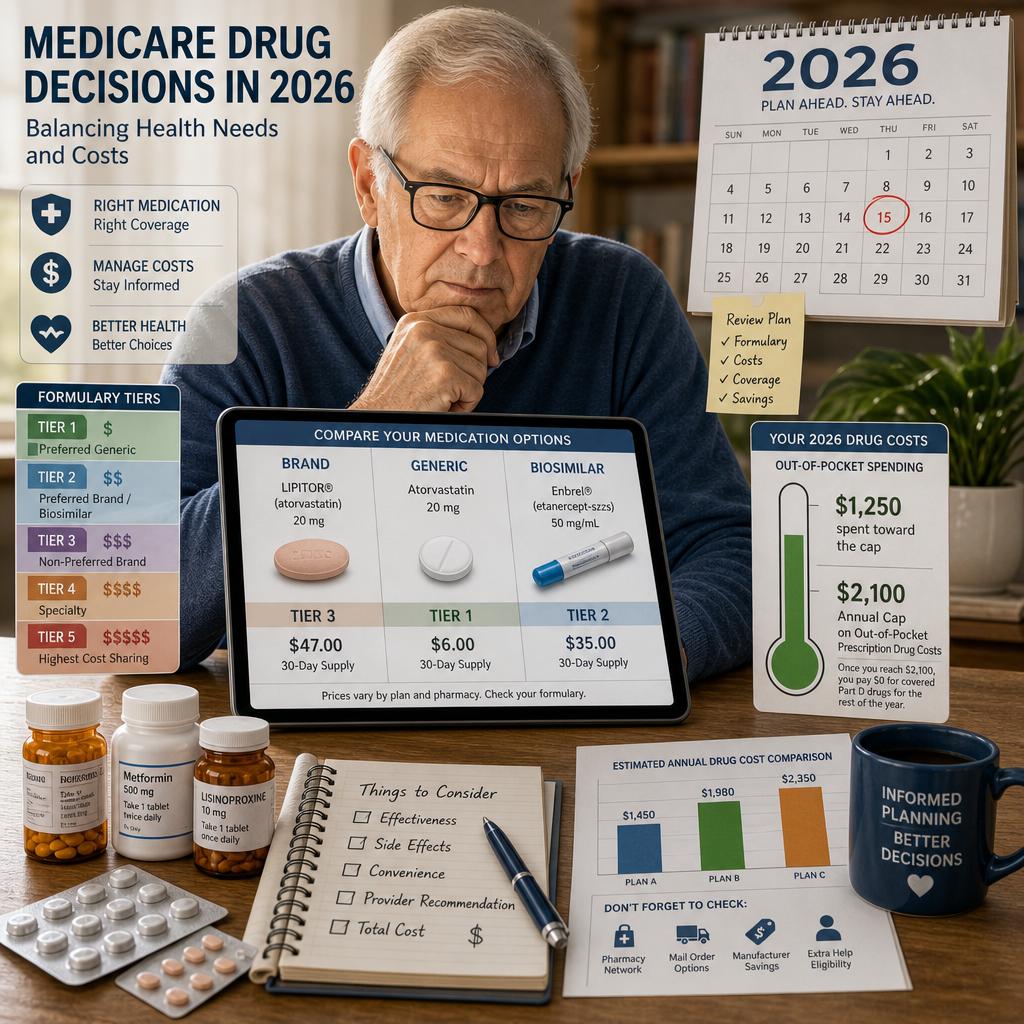
The new Medicare drug environment gives retirees more protection than they had just a few years ago. Medicare drug coverage now caps yearly out of pocket spending for covered Part D drugs at $2,100 in 2026, after which beneficiaries pay no copayment or coinsurance for covered Part D drugs for the rest of the calendar year . That is a meaningful improvement, especially for people taking cancer medications, autoimmune therapies, insulin alternatives, inhalers, anticoagulants, or other expensive prescriptions. Yet the cap does not eliminate the need to choose wisely. It only changes where the planning risk begins.
Why The 2026 Part D Cap Does Not Make Drug Selection Automatic
Consider a retiree named Elaine who takes a biologic medication for rheumatoid arthritis. Her physician says a biosimilar may be clinically appropriate. Her pharmacist says the plan prefers it. Her neighbor says the brand version worked better. Elaine is not simply choosing between two labels. She is choosing among formulary placement, pharmacy rules, prior authorization, step therapy, clinical comfort, and the timing of her own cash flow.
Medicare explains that actual drug costs vary based on whether prescriptions are on the plan formulary, what tier the drug occupies, which benefit phase the beneficiary is in, which pharmacy is used, and whether Extra Help applies . That means a biosimilar can be less expensive in one plan and surprisingly inconvenient in another. A generic can be preferred at one pharmacy and less favorable at a different one. A brand drug can be covered, but only after the prescriber documents why alternatives are not appropriate.
The Formulary Is The Real Contract
A formulary is not just a drug list. It is the operating manual for how your plan will treat your medication in real life. Medicare defines a formulary as the list of prescription drugs covered by a prescription drug plan or another insurance plan offering prescription drug benefits . The understated danger is that being on the formulary is only the first layer of protection. The tier, restrictions, pharmacy network, and refill rules can matter just as much.
This is where many well intentioned retirees get caught. They check whether a drug is covered, but not whether it is covered comfortably. A medication may be on the formulary but placed on a higher tier, subject to prior authorization, or more affordable only at a preferred pharmacy. Medicare notes that drug costs can differ depending on whether the pharmacy offers preferred or standard cost sharing, is out of network, or uses mail order . In a year when drug prices and negotiated pricing are changing, that level of detail is not clerical. It is financial planning.
Generics And Biosimilars Can Help But They Need Clinical Context
Medicare encourages beneficiaries to explore lower cost options, including choosing generics over brand name drugs or biosimilars over brand name biologic drugs, while also advising patients to check with their doctor to make sure the alternative is best for them . That final phrase matters. A biosimilar may be highly appropriate, but a person who has been stable for years on a biologic may need the prescriber to weigh disease control, side effects, administration method, and medical history before making a switch.
The same caution applies to generics. Most generics work beautifully and save money, but Medicare decisions should not be made by price alone. A beneficiary with narrow therapeutic needs, multiple drug allergies, swallowing difficulty, or complex dosing may need a specific formulation. If a plan favors one version while the clinician favors another, the beneficiary may need a coverage determination, exception request, or a carefully documented medical rationale rather than a quick pharmacy counter decision.
When Paying Outside The Plan Becomes Tempting
One of the more subtle 2026 decisions involves discount cards and pharmacy savings programs. Medicare acknowledges that beneficiaries might pay for a drug without insurance, such as by using pharmacy savings programs or manufacturer discounts, and suggests asking the pharmacist whether a less expensive option is available . That can be smart for a low cost medication. It can also be shortsighted for someone trying to move toward the annual Part D out of pocket cap.
The reason is simple but often missed. The $2,100 cap applies to out of pocket costs for drugs covered by the plan, with certain payments counted toward the limit . If a beneficiary repeatedly bypasses the plan to pay cash, those payments may not help in the way the person expects. A $9 cash price may be reasonable for a short term antibiotic. It may be less strategic for a recurring medication if using the plan helps track spending toward the cap, confirms formulary use, and preserves a paper trail for future exceptions.
The One Question To Ask Before Switching A Medication In 2026
Before accepting a substitution, beneficiaries should ask one disciplined question: How will this change affect my total year, not just today’s refill? That question forces the conversation to include the drug tier, the preferred pharmacy, any authorization rules, the prescriber’s clinical view, whether the medication counts under the plan benefit, and how close the beneficiary may come to the $2,100 Part D cap.
This is especially important for people in Medicare Advantage plans that include drug coverage. Medicare Advantage often bundles Part A, Part B, and usually Part D into one private plan structure, and many plans include drug coverage rather than requiring a separate Part D plan . That convenience can be valuable, but it also means the drug decision is tied to the broader plan decision. A plan with attractive dental or vision extras may still be a poor fit if it handles a specialty medication unfavorably.
Why Professional Review Matters More In A Capped Drug Year
The 2026 Part D cap creates a false sense of simplicity. Yes, it limits covered Part D drug exposure. No, it does not guarantee that every drug version is covered, that every pharmacy prices the same way, or that a substitution is clinically appropriate. Medicare also makes clear that plan coverage and costs can change each year, which is why beneficiaries should review health and drug coverage annually rather than assume last year’s choice still fits .
Vista Mutual approaches this as a practical risk review, not a brochure comparison. We look at the medications you actually take, the pharmacies you actually use, the doctors you do not want to lose, and the tradeoffs between Medicare Advantage, Supplement, and Part D designs. In 2026, the best drug decision is rarely just the cheapest refill. It is the coverage path that protects your health, your access, and your financial predictability over the full year.
If you want confidence before changing a medication, plan, pharmacy, or coverage strategy, Consult with the Vista Mutual team. Professional guidance can turn a confusing set of drug rules into a clear Medicare plan built around your real life.